Download presentation
1
Journal Club 2009年4月30日 8:30-8:55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科
Ryuzo Kawamori, Naoko Tajima, Yasuhiko Iwamoto, Atsunori Kashiwagi, Kazuaki Shimamoto, Kohei Kaku, on behalf of the Voglibose Ph-3 Study Group Voglibose for prevention of type 2 diabetes mellitus: a randomised, double-blind trial in Japanese individuals with impaired glucose tolerance Published online April 22, 2009 DOI: /S (09) Bakris GL, Toto RD, McCullough PA, Rocha R, Purkayastha D, Davis P; GUARD (Gauging Albuminuria Reduction With Lotrel in Diabetic Patients With Hypertension) Study Investigators. Effects of different ACE inhibitor combinations on albuminuria: results of the GUARD study. Kidney Int Jun;73(11): 2009年4月30日 8:30-8:55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi
 Bakris GL, Toto RD, McCullough PA, Rocha R, Purkayastha D, Davis P; GUARD (Gauging Albuminuria Reduction With Lotrel in Diabetic Patients With Hypertension) Study Investigators. Effects of different ACE inhibitor combinations on albuminuria: results of the GUARD study. Kidney Int Jun;73(11): 年4月30日 8:30-8:55. 8階 医局. 埼玉医科大学 総合医療センター 内分泌・糖尿病内科. Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University. 松田 昌文. Matsuda, Masafumi.")
2
Department of Medicine, Metabolism and Endocrinology, Juntendo University School of Medicine, Tokyo, Japan (Prof R Kawamori MD); Division of Diabetes, Metabolism and Endocrinology, Department of Internal Medicine, Jikei University School of Medicine, Tokyo, Japan (Prof N Tajima MD); Diabetes Centre, Department of Medicine, Tokyo Women’s Medical University, Tokyo, Japan (Prof Y Iwamoto MD); Department of Medicine, Shiga University of Medical Science, Shiga, Japan (Prof A Kashiwagi MD); Second Department of Internal Medicine, Sapporo Medical University, Sapporo, Japan (Prof K Shimamoto MD); and Diabetes and Endocrine Division, Department of Medicine, Kawasaki Medical School, Kurashiki, Japan (Prof K Kaku MD) Published online April 22, 2009 DOI: /S (09)
")
3
April 25, 2009 at Granvia Hotel Okayama

4
Background The increased prevalence of type 2 diabetes mellitus is a major concern for health providers. We therefore assessed whether voglibose, an α-glucosidase inhibitor, could prevent the development of type 2 diabetes in high-risk Japanese individuals with impaired glucose tolerance.

5
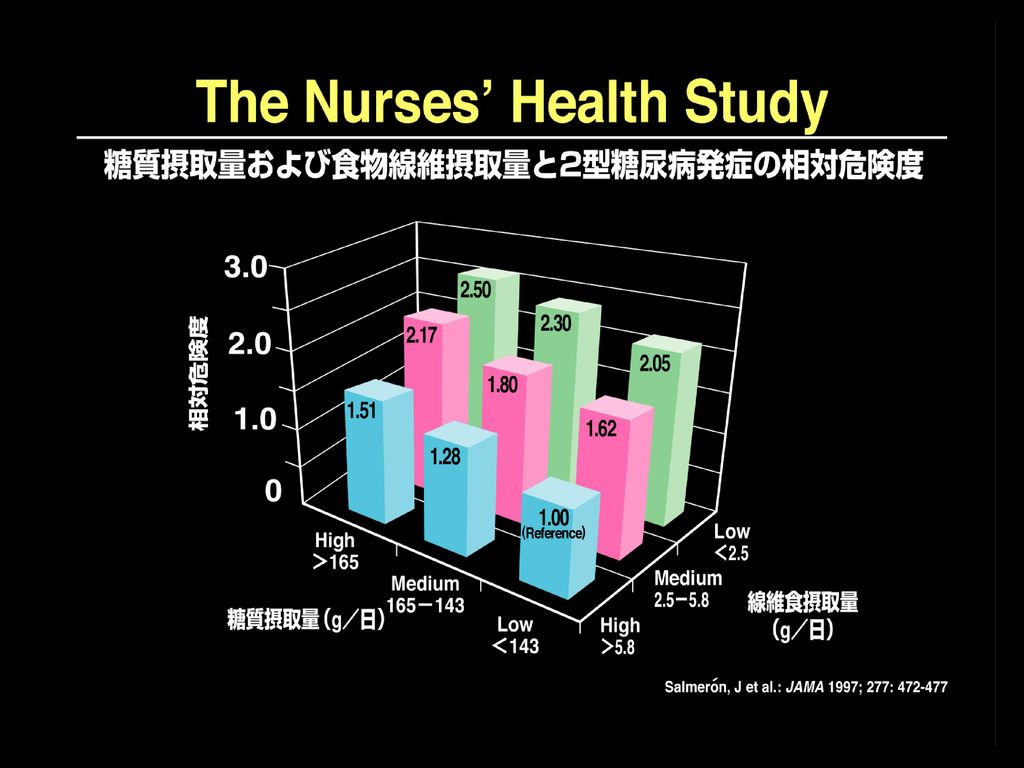
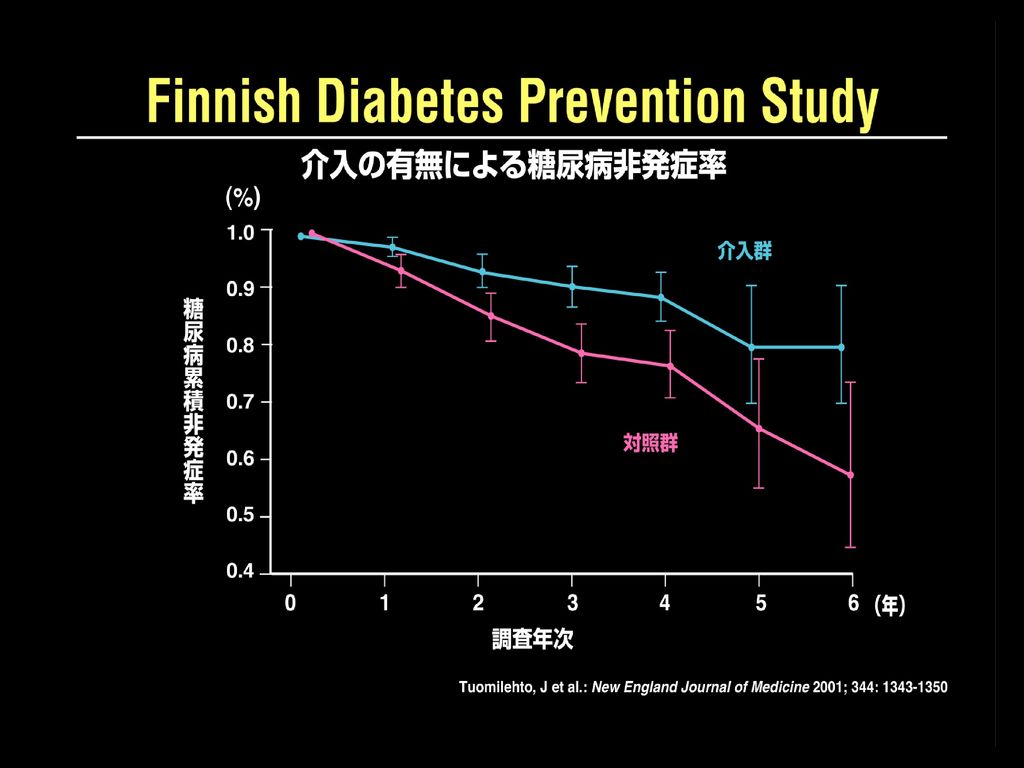
Primary Prevention of Type 2 Diabetes Mellitus
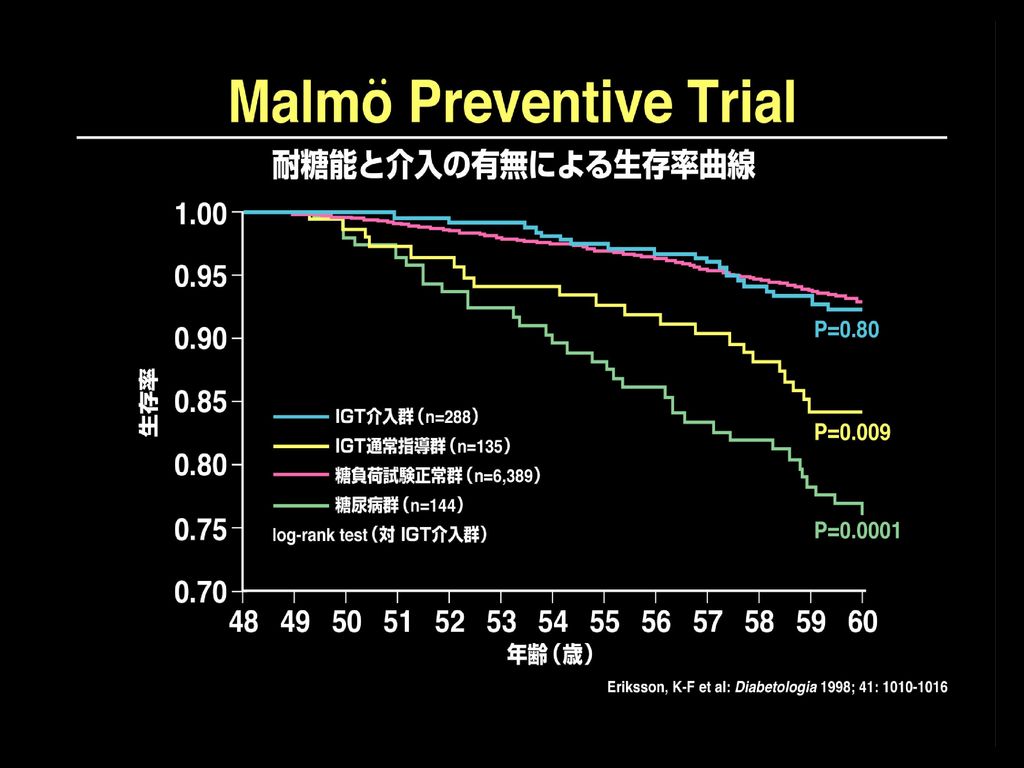
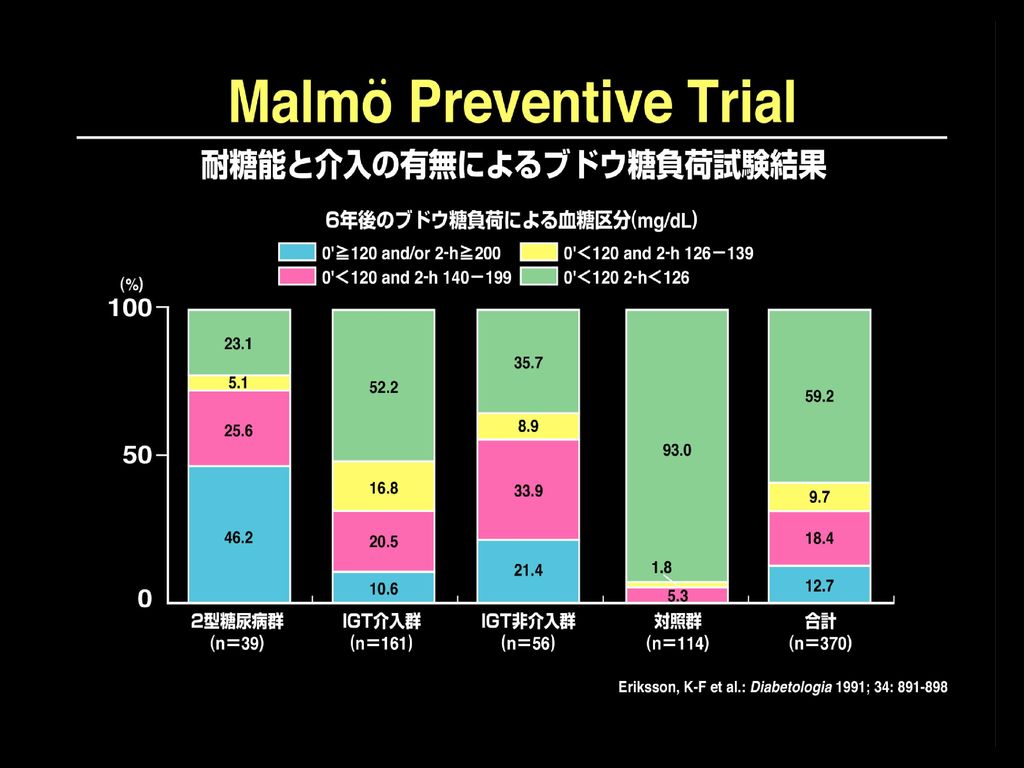
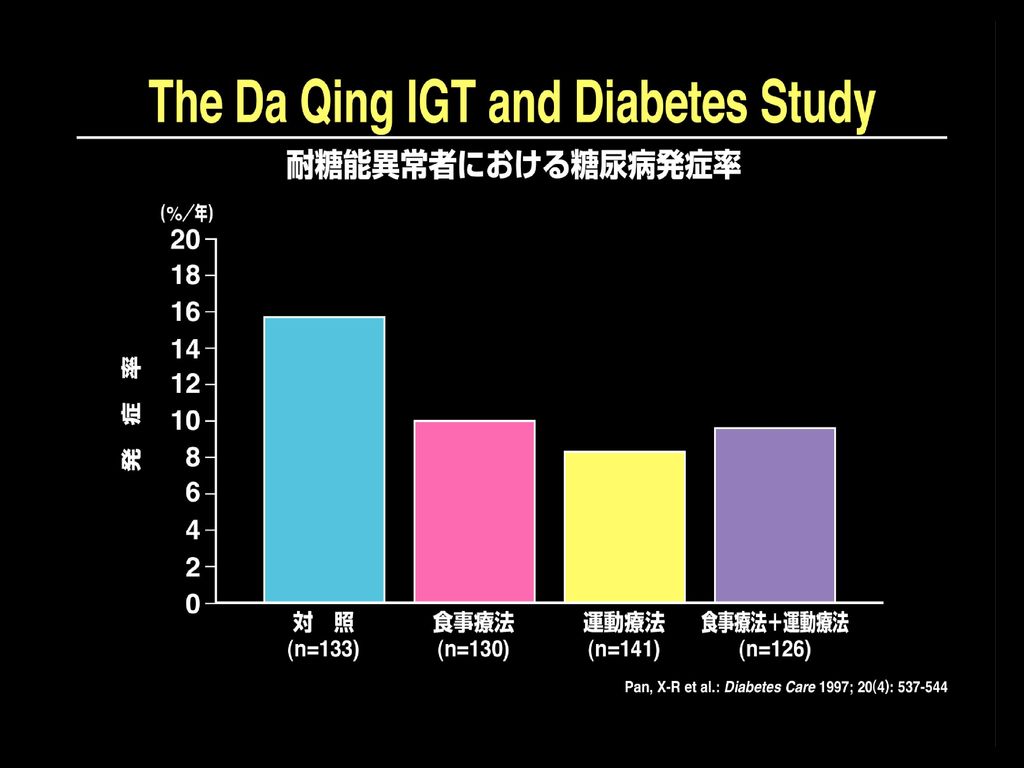
● Life style modification ・Malmö feasibility study (Eriksson, 1991) ・Malmö Prfevention Trial (Eriksson, 1998) ・DaQing IGT and Diabetes Study (Pan, 1997) ・Finnish Diabetes Prevnetion Study (Tuomilehto, 2001) ・Japan Diabetes Prevention Study (Kuzuya, on going) ・Stockholm Diabetes Prevention Program (Bjärås, on going) ● Drug intervention ・Diabetes Prevention Program (DPP Research Group, 2002) ・STOP-NIDDM (Chiasson, 2002) ・TRIPOD (Buchanan, 2001) ・EDIT (Holman, 2003) ・NAVIGATOR (on going) ・DREAM (Boche, 2006) ・ACT NOW (DeFronzo,2008) ・ONTARGET (ONTARGET group, 2008) STOP-NIDDM:Study To Prevent NDDM, TRIPOD:Troglitazone In Prevention of Diabetes EDIT:Early Diabetes Intervention Trial, NAVIGATOR:Natglinide and Valsartan in Impaired Glucose Tolerance Outcome Reaserach DREAM:Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medications
 ・Malmö Prfevention Trial (Eriksson, 1998) ・DaQing IGT and Diabetes Study (Pan, 1997) ・Finnish Diabetes Prevnetion Study (Tuomilehto, 2001) ・Japan Diabetes Prevention Study (Kuzuya, on going) ・Stockholm Diabetes Prevention Program (Bjärås, on going) ● Drug intervention. ・Diabetes Prevention Program (DPP Research Group, 2002) ・STOP-NIDDM (Chiasson, 2002) ・TRIPOD (Buchanan, 2001) ・EDIT (Holman, 2003) ・NAVIGATOR (on going) ・DREAM (Boche, 2006) ・ACT NOW (DeFronzo,2008) ・ONTARGET (ONTARGET group, 2008) STOP-NIDDM:Study To Prevent NDDM, TRIPOD:Troglitazone In Prevention of Diabetes. EDIT:Early Diabetes Intervention Trial, NAVIGATOR:Natglinide and Valsartan in Impaired Glucose Tolerance Outcome Reaserach. DREAM:Diabetes Reduction Assessment with Ramipril and Rosiglitazone Medications.")
6
Prevention of Diabetes Mellitus
ONTARGET ARB ACEI ONTARGET ARB+ACEI ACEI TRANSCEND ARB placebo 松田昌文:DREAM study 内分泌・糖尿病科 26(1):35-41,
:35-41,")
7
Prevention of Diabetes Mellitus
ACTNOW Pioglitazone Placebo 松田昌文:DREAM study 内分泌・糖尿病科 26(1):35-41,
:35-41,")
12
Lancet 2008; 371: 1783–89

15
糖尿病予防研究 (米国) 31%less 58%less 各群約1000人
 31%less 58%less 各群約1000人")
16
追跡期間中におけるメタボリックシンドローム累積発症率
糖尿病予防研究 (米国) 追跡期間中におけるメタボリックシンドローム累積発症率 60 17%less 45 41%less 累積発症率 30 15 各群約500人
 追跡期間中におけるメタボリックシンドローム累積発症率 %less %less. 累積発症率 各群約500人.")
17
アクトスの糖尿病発症予防効果(PIPOD Study)
(%) 60 プラセボ群(TRIPOD) 累積糖尿病発症率 40 こちらは、PIPOD(パイポッド) Study:The Pioglitazone in Prevention of Diabetesという試験の結果です。 妊娠糖尿病既往例におけるトログリタゾンの糖尿病発症予防効果を検討したTRIPOD(トライポッド) Study:The Troglitazone in Prevention of Diabetesのうち、試験中止後、糖尿病を発症していなかった89例を対象に、3年間にわたりアクトス(45mg/日)の糖尿病発症予防効果をみました。 アクトスを投与した群の糖尿病発症率は4.6%/年で、TRIPOD Studyにおけるトログリタゾンの5.4%/年と同等の糖尿病発症予防効果を認めました。 今回のPIPOD Studyではプラセボ群がありませんが、アクトス群の糖尿病発症率が4.6%/年とトログリタゾン群の発症率とほぼ同等であったことから、アクトスにも糖尿病発症予防効果があると結論されています。 演者は、アクトスが糖尿病の発症を防いだ理由として、インスリン分泌不全の傾向があるため糖尿病を発症しやすい妊娠糖尿病既往例に対して、インスリン抵抗性を改善することで膵β細胞を『休息(Rest)』させることによるものと結論しています。 参考)TRIPOD Studyとは 妊娠糖尿病既往例をトログリタゾン群とプラセボ群に分け、糖尿病発症予防効果を比較した試験です。トログリタゾン群の糖尿病発症率は5.4%/年で、プラセボ群の12.1%/年に比べて低く、糖尿病発症の相対リスクを55%低下させました。また、トログリタゾン投薬中止後も観察を続けたところ、両群間の糖尿病発症率はさらに差を認め、トログリタゾンの投与を受けていた群はプラセボ群に比べて、糖尿病発症の相対リスクを92%低下させました。 トログリタゾン群(TRIPOD) 20 ピオグリタゾン群(PIPOD) 年間発症率:4.6%/年 1 2 3 4 5 (年) 観察期間 妊娠糖尿病既往例におけるトログリタゾンの糖尿病発症予防効果を検討したTRIPOD Studyのうち、試験中止後、糖尿病を発症していなかった89例を対象に3年間にわたるアクトス(45mg/日)の糖尿病発症予防効果をみた。 Buchanan T. et al.: 65th ADA Scientific Sessions,2005.
 60. プラセボ群(TRIPOD) 累積糖尿病発症率. 40. こちらは、PIPOD(パイポッド) Study:The Pioglitazone in Prevention of Diabetesという試験の結果です。 妊娠糖尿病既往例におけるトログリタゾンの糖尿病発症予防効果を検討したTRIPOD(トライポッド) Study:The Troglitazone in Prevention of Diabetesのうち、試験中止後、糖尿病を発症していなかった89例を対象に、3年間にわたりアクトス(45mg/日)の糖尿病発症予防効果をみました。 アクトスを投与した群の糖尿病発症率は4.6%/年で、TRIPOD Studyにおけるトログリタゾンの5.4%/年と同等の糖尿病発症予防効果を認めました。 今回のPIPOD Studyではプラセボ群がありませんが、アクトス群の糖尿病発症率が4.6%/年とトログリタゾン群の発症率とほぼ同等であったことから、アクトスにも糖尿病発症予防効果があると結論されています。 演者は、アクトスが糖尿病の発症を防いだ理由として、インスリン分泌不全の傾向があるため糖尿病を発症しやすい妊娠糖尿病既往例に対して、インスリン抵抗性を改善することで膵β細胞を『休息(Rest)』させることによるものと結論しています。 参考)TRIPOD Studyとは. 妊娠糖尿病既往例をトログリタゾン群とプラセボ群に分け、糖尿病発症予防効果を比較した試験です。トログリタゾン群の糖尿病発症率は5.4%/年で、プラセボ群の12.1%/年に比べて低く、糖尿病発症の相対リスクを55%低下させました。また、トログリタゾン投薬中止後も観察を続けたところ、両群間の糖尿病発症率はさらに差を認め、トログリタゾンの投与を受けていた群はプラセボ群に比べて、糖尿病発症の相対リスクを92%低下させました。 トログリタゾン群(TRIPOD) 20. ピオグリタゾン群(PIPOD) 年間発症率:4.6%/年 (年) 観察期間. 妊娠糖尿病既往例におけるトログリタゾンの糖尿病発症予防効果を検討したTRIPOD Studyのうち、試験中止後、糖尿病を発症していなかった89例を対象に3年間にわたるアクトス(45mg/日)の糖尿病発症予防効果をみた。 Buchanan T. et al.: 65th ADA Scientific Sessions,2005.")
18
ACTos NOW Study for the Prevention of Diabetes (ACT NOW) Study
試験対象者の内訳 スクリーニング(1,850例) IGT*(602例) IFG/IGT(407例) Isolated IGT(195例) IGT( Impaired glucose tolerance):1回のOGTTにより2時間血糖値が140~199mg/dLを示す アクトスの効能・効果は2型糖尿病です De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.
 IGT*(602例) IFG/IGT(407例) Isolated IGT(195例) IGT( Impaired glucose tolerance):1回のOGTTにより2時間血糖値が140~199mg/dLを示す. アクトスの効能・効果は2型糖尿病です. De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.")
19
ACT NOW ~インスリン感受性への影響~
Matsuda(0-120)index FSIVGTTによるSI (%/分) 10 5 p<0.001 8 4 6 3 4 2 2 1 投与前 投与後 投与前 投与後 投与前 投与後 投与前 投与後 プラセボ ピオグリタゾン プラセボ ピオグリタゾン アクトスの効能・効果は2型糖尿病です IGT患者600例をアクトス45mg/日またはプラセボに割り付け、二重盲検下で2型糖尿病の発症を4年にわたり検討した。 De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.
index. FSIVGTTによるSI. (%/分) p< 投与前. 投与後. 投与前. 投与後. 投与前. 投与後. 投与前. 投与後. プラセボ. ピオグリタゾン. プラセボ. ピオグリタゾン. アクトスの効能・効果は2型糖尿病です. IGT患者600例をアクトス45mg/日またはプラセボに割り付け、二重盲検下で2型糖尿病の発症を4年にわたり検討した。 De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.")
20
ACT NOW ~インスリン抵抗性に対する膵β細胞の代償能への影響~
I/G x Matsuda(0-120) AIR x SI p<0.005 6 p<0.005 1200 5 4 800 3 2 400 1 投与前 投与後 投与前 投与後 投与前 投与後 投与前 投与後 プラセボ ピオグリタゾン プラセボ ピオグリタゾン アクトスの効能・効果は2型糖尿病です IGT患者600例をアクトス45mg/日またはプラセボに割り付け、二重盲検下で2型糖尿病の発症を4年にわたり検討した。 De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.
 AIR x SI. p< p< 投与前. 投与後. 投与前. 投与後. 投与前. 投与後. 投与前. 投与後. プラセボ. ピオグリタゾン. プラセボ. ピオグリタゾン. アクトスの効能・効果は2型糖尿病です. IGT患者600例をアクトス45mg/日またはプラセボに割り付け、二重盲検下で2型糖尿病の発症を4年にわたり検討した。 De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.")
21
ACT NOW ~糖尿病発症抑制~ 6.8%/年 1.5%/年 NNT(1年間)=3.5 ハザード比 0.19 95%CI
0.3 NNT(1年間)=3.5 6.8%/年 ハザード比 0.19 95%CI 0.09,0.39 p値 累積ハザード 0.25 0.2 プラセボ 0.15 0.10 1.5%/年 0.05 ピオグリタゾン 10 20 30 40 50 (ヵ月) 症例数 プラセボ ピオグリタゾン 観察期間 アクトスの効能・効果は2型糖尿病です IGT患者600例をアクトス45mg/日またはプラセボに割り付け、二重盲検下で2型糖尿病の発症を4年にわたり検討した。 De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.
= %/年. ハザード比 %CI. 0.09,0.39. p値 累積ハザード プラセボ %/年 ピオグリタゾン (ヵ月) 症例数. プラセボ ピオグリタゾン 観察期間. アクトスの効能・効果は2型糖尿病です. IGT患者600例をアクトス45mg/日またはプラセボに割り付け、二重盲検下で2型糖尿病の発症を4年にわたり検討した。 De Fronzo R.A.:ADA 68th Scientific Sessions,2008,San Francisco.")
22
α-グルコシダーゼ阻害薬の作用 腸 管 内 でんぷん 蔗糖 -でんぷん アミラーゼ 众所周知,糖物质是由单糖聚合而成的。作为多聚糖的淀粉被唾液、胰液中的α-淀粉酶分解成三聚糖、二聚糖,被小肠粘膜上存在的α-葡萄糖苷酶最终分解成单糖以后才能被吸收。二聚糖(砂糖)可直接被α-葡萄糖苷酶分解为葡萄糖和果糖以后被吸收。 α-GI口服以后到达小肠,竞争阻断α-葡萄糖苷酶,而起到延迟糖物质的消化吸收。 小腸上皮 絨毛膜 α-glucosidase α-glucosidase a-glucosidase阻害薬 吸収 移送 ぶどう糖 果糖 ぶどう糖 後藤 由夫:nanoGIGA, 3(4), 598, 1994.
可直接被α-葡萄糖苷酶分解为葡萄糖和果糖以后被吸收。 α-GI口服以后到达小肠,竞争阻断α-葡萄糖苷酶,而起到延迟糖物质的消化吸收。 小腸上皮. 絨毛膜. α-glucosidase. α-glucosidase. a-glucosidase阻害薬. 吸収. 移送. ぶどう糖. 果糖. ぶどう糖. 後藤 由夫:nanoGIGA, 3(4), 598,")
23
α-グルコシダーゼ阻害薬のぶどう糖吸収抑制
α-GI経口服用時 血 糖 時間 糖 十二指腸 空腸 回腸 大腸 正常のぶどう糖の吸収 血 糖 時間 糖 十二指腸 空腸 回腸 大腸 下面请看α-GI作用模式图。 正常状态下,糖类物质在小肠上部(十二指肠、空肠)迅速被消化吸收,所以,餐后血糖急剧升高。 但是,餐前口服α-GI,可有效抑制小肠上部血糖的迅速吸收,使糖物质缓慢吸收,从而控制餐后血糖过高。也就是说,餐后血糖不太高,而又能完全吸收糖类物质。 後藤 由夫 (東北厚生年金病院内科):PTM Vol.7, 4(2) FEB., 1995.
迅速被消化吸收,所以,餐后血糖急剧升高。 但是,餐前口服α-GI,可有效抑制小肠上部血糖的迅速吸收,使糖物质缓慢吸收,从而控制餐后血糖过高。也就是说,餐后血糖不太高,而又能完全吸收糖类物质。 後藤 由夫 (東北厚生年金病院内科):PTM Vol.7, 4(2) FEB.,")
24
Early Diabetes Intervention Trial
PI Prof. R. Holman, Univ. of Oxford Population IFG/IGT subjects; n= 631 (6 years follow-up) Endpoint Onset of diabetes (OGTT or FPG) Treatment: Metformin 500 mg tds, Acarbose 50 mg tds Placebo Metformin N=312 N=155 N=157 Acarbose + Metformin Acarbose N=319 N=160 N=159 N=315 N=316 Acarbose reduces the risk of developing type 2 diabetes in IGT by 34 % in the ITT analysis versus no effect of Metformin
 Endpoint Onset of diabetes (OGTT or FPG) Treatment: Metformin 500 mg tds, Acarbose 50 mg tds. Placebo. Metformin. N=312. N=155. N=157. Acarbose. + Metformin. Acarbose. N=319. N=160. N=159. N=315. N=316. Acarbose reduces the risk of developing type 2 diabetes in IGT by 34 % in the ITT analysis versus no effect of Metformin.")
25
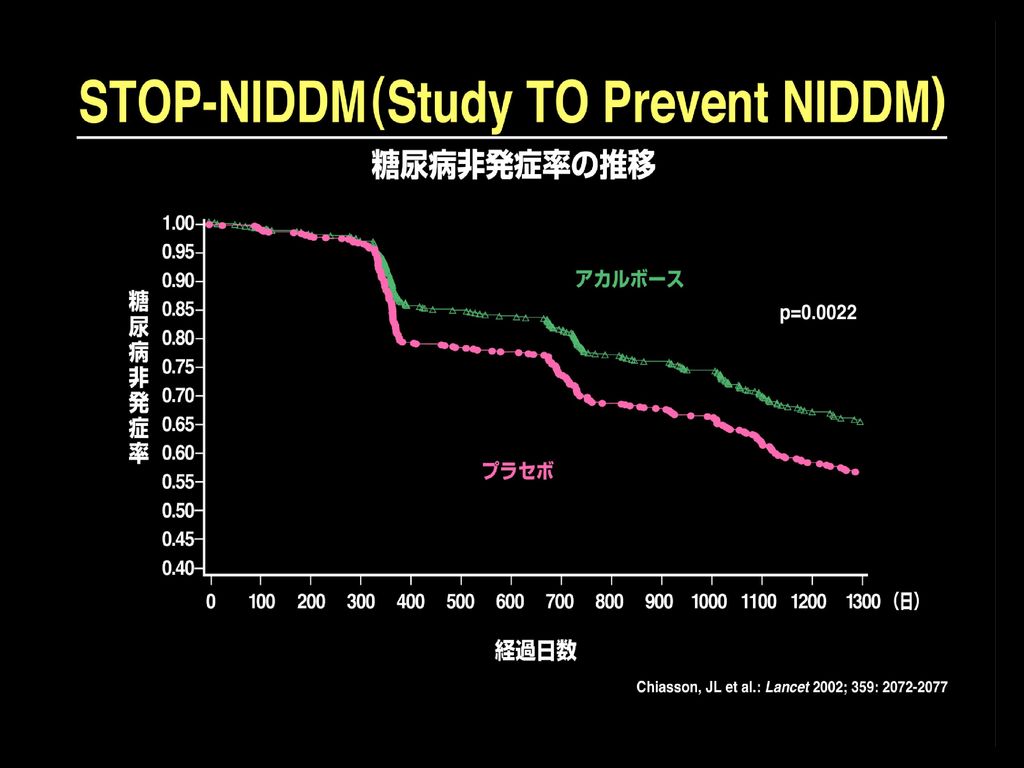
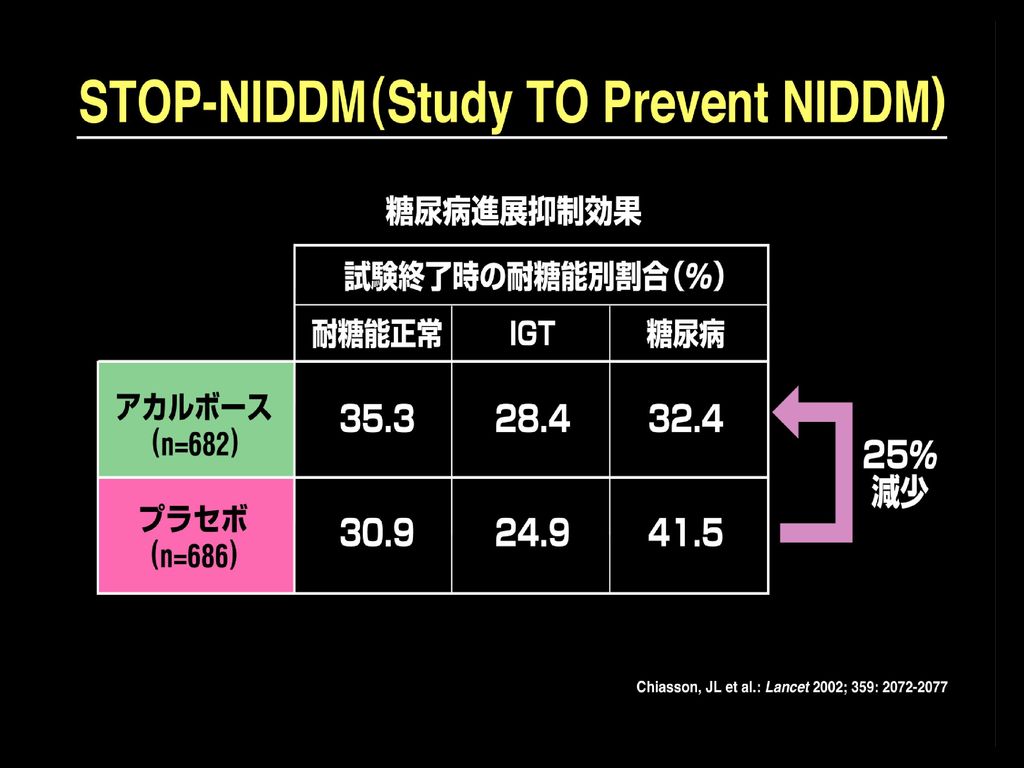
STOP-NIDDM 参加国及び研究者 9カ国40施設で実施
カナダ ドイツ オーストリア スペイン イスラエル フィンランド ノルウェー スウェーデン デンマーク STOP-NIDDM参加国及び研究者 STOP-NIDDMはカナダ、ドイツ、オーストリア、ノルウェー、デンマーク、スウェーデン、フィンランド、イスラエル及びスペインで実施された多施設二重盲検プラセボ対照無作為化試験です。モントリオール大学のJean-Louis Chiasson教授を主任研究者とし、その他各国の研究者から成るSTOP-NIDDM Trial Research Groupにより実施されました。 Principal Investigator: Chiasson J-L (カナダ) Steering Committee: Josse R (カナダ) Hanefeld M (ドイツ) Laakso M (フィンランド) Gomis R (スペイン) Karasik A (イスラエル)
 Steering Committee: Josse R (カナダ) Hanefeld M (ドイツ) Laakso M (フィンランド) Gomis R (スペイン) Karasik A (イスラエル)")
26
STOP-NIDDM 試験プロファイル n = 14,742 選択基準による選定 除外者 n = 13,313 試験基準の非適格者
アカルボース群 n = 1,429 無作為割り付け n = 715 プラセボ群 STOP-NIDDMの試験のプロファイル STOP-NIDDMの試験のプロファイルです。 IGTを有する1,429例の被験者が無作為にアカルボース群(n=714)、プラセボ群(n=715)に割り付けられました。 このうち567例(40%)がカナダ、382例(27%)がドイツとオーストリア、334例(24%)が北欧諸国、そしてスペインとイスラエルからそれぞれ73例(5%)でした。17例(アカルボース群8例、プラセボ群9例)はIGTではないと判断され、除外されました。さらに44例(アカルボース群24例、プラセボ群20例)は無作為化後の適切なデータがなかったため除外されました。およそ4分の1が試験途中で脱落し、この半数(48%)は1年目に脱落しました。投与を中止 した最も高頻度で唯一の理由は消化器系副作用でした。これら被験者すべてに対し、3年後にOGTTを含め、評価項目パラメータが測定されています。 n=32 除外 n= IGT基準に 合致せず n=24 無作為化後の データ無し n=29 除外 n= IGT基準に 合致せず n=20 無作為化後の データ無し n=211 早期に脱落 n=130 早期に脱落 n = 682 解析対象 n = 686 (ITT) 解析対象 Chiasson JL, et al. Lancet ;359::2072–2077,2002..
、プラセボ群(n=715)に割り付けられました。 このうち567例(40%)がカナダ、382例(27%)がドイツとオーストリア、334例(24%)が北欧諸国、そしてスペインとイスラエルからそれぞれ73例(5%)でした。17例(アカルボース群8例、プラセボ群9例)はIGTではないと判断され、除外されました。さらに44例(アカルボース群24例、プラセボ群20例)は無作為化後の適切なデータがなかったため除外されました。およそ4分の1が試験途中で脱落し、この半数(48%)は1年目に脱落しました。投与を中止. した最も高頻度で唯一の理由は消化器系副作用でした。これら被験者すべてに対し、3年後にOGTTを含め、評価項目パラメータが測定されています。 n=32 除外. n=8 IGT基準に. 合致せず. n=24 無作為化後の. データ無し. n=29 除外. n=9 IGT基準に. 合致せず n=20 無作為化後の. データ無し. n=211 早期に脱落. n=130 早期に脱落. n = 682 解析対象. n = 686 (ITT) 解析対象. Chiasson JL, et al. Lancet ;359::2072–2077,")
27
試験デザイン 経過月数 Placebo 来院 –1 6 12 18 24 30 36 60 プラセボ 1日3回 (n=715) プラセボ
STOP NIDDM 試験デザイン 経過月数 –1 6 12 18 24 30 36 60 プラセボ 1日3回 (n=715) プラセボ (n=1,429) 試験デザイン 無作為二重盲検法によりグルコバイ錠投与群またはプラセボ投与群に割り付け、心血管イベントの発症等について平均3.3年間追跡しました。グルコバイ錠50mg/日から投与開始し、忍容性を確認しながら徐々に最大100mg×3日まで増量しました。なお、アカルボース群での平均1日量は194±87mgでした。 被験者に体重減量または体重維持の食事療法、規則的な運動療法の指導が行われました。全被験者は薬剤数の確認と調剤、有害事象の記録および空腹時血糖測定のため3ヶ月毎に看護師の面接を受け、6ヶ月毎に治験医師の診察を受けています。最後の被験者が3年間の治療を終えるまで、試験を継続しました。投与期間終了後に糖尿病を発症しなかった全被験者について、単純盲検法でプラセボを投与して3ヶ月間追跡観察し、再び同様の測定を行っています。 全被験者に対し1年毎に75gOGTTを実施し、3ヶ月毎の受診時の空腹時血糖が126mg/dL以上となった場合は自動的にOGTTを行いました。一次エンドポイントに到達した被験者もなお試験の対象者として二重盲検下で試験薬の投与を継続し、他の糖尿病用薬の追加投与の必要がない限り、OGTTを毎年実施しました。 3ヵ月間 プラセボ Placebo アカルボース 100mg 1日3回 (n=714) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 終了 来院 Chiasson JL, et al. Lancet ;359::2072–2077,2002..
 プラセボ. (n=1,429) 試験デザイン. 無作為二重盲検法によりグルコバイ錠投与群またはプラセボ投与群に割り付け、心血管イベントの発症等について平均3.3年間追跡しました。グルコバイ錠50mg/日から投与開始し、忍容性を確認しながら徐々に最大100mg×3日まで増量しました。なお、アカルボース群での平均1日量は194±87mgでした。 被験者に体重減量または体重維持の食事療法、規則的な運動療法の指導が行われました。全被験者は薬剤数の確認と調剤、有害事象の記録および空腹時血糖測定のため3ヶ月毎に看護師の面接を受け、6ヶ月毎に治験医師の診察を受けています。最後の被験者が3年間の治療を終えるまで、試験を継続しました。投与期間終了後に糖尿病を発症しなかった全被験者について、単純盲検法でプラセボを投与して3ヶ月間追跡観察し、再び同様の測定を行っています。 全被験者に対し1年毎に75gOGTTを実施し、3ヶ月毎の受診時の空腹時血糖が126mg/dL以上となった場合は自動的にOGTTを行いました。一次エンドポイントに到達した被験者もなお試験の対象者として二重盲検下で試験薬の投与を継続し、他の糖尿病用薬の追加投与の必要がない限り、OGTTを毎年実施しました。 3ヵ月間. プラセボ. Placebo. アカルボース 100mg 1日3回 (n=714) 終了. 来院. Chiasson JL, et al. Lancet ;359::2072–2077,")
30
アカルボースの高血圧発症抑制 血圧 ³140/90mmHg を高血圧とする STOP NIDDM 0.20 0.18 累積発症率 0.16
0.14 プラセボ 0.12 0.10 アカルボースの高血圧発症抑制 アカルボース群、プラセボ群における新規に高血圧の累積発症率を示したものです。割り付け後早期の段階で高血圧の発症率に差が見られ始め、その差は開き続けています。アカルボースによる治療は高血圧症の発症リスクに対して有意な効果を発揮しました。(p= Log-rank検定) 0.08 0.06 アカルボース 0.04 0.02 p=0.007 (Log-Rank Test) p=0.006 (Cox Proportional Model) 0.00 100 200 300 400 500 600 700 800 900 1000 1100 1200 1300 1400 無作為化後経過日数 プラセボ アカルボース 686 682 663 645 646 617 632 601 607 585 593 570 581 559 573 559 562 552 550 524 538 514 458 435 368 342 287 254 196 178 Chiasson JL, et al. JAMA 290: 486–494,2003.
 アカルボース p=0.007 (Log-Rank Test) p=0.006 (Cox Proportional Model) 無作為化後経過日数. プラセボ. アカルボース Chiasson JL, et al. JAMA 290: 486–494,2003.")
31
アカルボースの心血管イベントの発症抑制 (初回のイベントのみ) STOP NIDDM 0.06 累積発症率 0.05 0.04 0.03
アカルボースの心血管イベントの発症抑制(初回のイベントのみ) アカルボース群、プラセボ群での心血管イベントの累積発症率の比較データです。アカルボース群ではプラセボ群に比べ心血管イベントの累積発症率が有意に低いことが示されました(p=0.04 log-rank検定)。 Cox比例モデルによると、アカルボースはプラセボに比べ、心血管イベントのハザード比が0.51(95%CI, ; p=0.03)と、発症リスクを有意に低下させました。 プラセボ 0.02 アカルボース 0.01 p=0.04 (Log-Rank Test) p=0.03 (Cox Proportional Model) 0.00 100 200 300 400 500 600 700 800 900 1000 1100 1200 1300 1400 無作為化後経過日数 プラセボ アカルボース 686 682 675 659 667 635 658 622 643 608 638 601 633 596 527 590 615 577 611 567 604 558 519 473 424 376 332 286 232 203 Chiasson JL, et al. JAMA 290: 486–494,2003.
 アカルボース群、プラセボ群での心血管イベントの累積発症率の比較データです。アカルボース群ではプラセボ群に比べ心血管イベントの累積発症率が有意に低いことが示されました(p=0.04 log-rank検定)。 Cox比例モデルによると、アカルボースはプラセボに比べ、心血管イベントのハザード比が0.51(95%CI, ; p=0.03)と、発症リスクを有意に低下させました。 プラセボ アカルボース p=0.04 (Log-Rank Test) p=0.03 (Cox Proportional Model) 無作為化後経過日数. プラセボ. アカルボース Chiasson JL, et al. JAMA 290: 486–494,2003.")
32
アカルボースの心血管イベント発症抑制 患者数 リスク 低下 (%) アカルボース プラセボ が優れる が優れる 心血管イベント
STOP NIDDM アカルボースの心血管イベント発症抑制 患者数 リスク 低下 (%) アカルボース プラセボ が優れる が優れる 心血管イベント アカルボース (n=682) プラセボ (n=686) P値 0.5 1.0 1.5 2.0 冠動脈疾患 心筋梗塞 狭心症 血行再建術 心血管死 うっ血性心不全 0 2 – 脳血管イベント/ 脳卒中 末梢血管障害 – 全ての心血管イベント 0.02 0.13 0.18 0.63 – 0.51 0.93 0.03 アカルボースの心血管イベント発症抑制 症候性の心筋梗塞はプラセボ群で12例であったのに対し、アカルボース群では1例と統計学的有意差が認められました(HR, 0.09; 95%CI, ; p=0.02)。その他の個々の心血管イベントについては、発症例数が少ないため有意な治療効果は認められませんでしたが、一貫してアカルボース治療の有用性を支持する傾向を示しました。 全ての心血管イベント発症を合計すると、プラセボ群では32例であったのに対し、アカルボース群では15例でした。アカルボースによる治療はIGT患者において心血管イベントの相対リスクを49%有意に低下させ、絶対リスクを2.5%低下させました。 さらに心血管イベントを起こした患者の72%(プラセボ群22例、アカルボース群12例)は、糖尿病発症前のIGTの段階で心血管イベントを経験しており、残りの28%(プラセボ群10例、アカルボース3例)は糖尿病発症後に心血管イベントを発症していました。 Chiasson JL, et al. JAMA 290: 486–494,2003.
 アカルボース プラセボ. が優れる が優れる. 心血管イベント. アカルボース. (n=682) プラセボ. (n=686) P値 冠動脈疾患. 心筋梗塞 狭心症 血行再建術 心血管死 うっ血性心不全 0 2 – 脳血管イベント/ 脳卒中 末梢血管障害 1 1 – 全ての心血管イベント – アカルボースの心血管イベント発症抑制. 症候性の心筋梗塞はプラセボ群で12例であったのに対し、アカルボース群では1例と統計学的有意差が認められました(HR, 0.09; 95%CI, ; p=0.02)。その他の個々の心血管イベントについては、発症例数が少ないため有意な治療効果は認められませんでしたが、一貫してアカルボース治療の有用性を支持する傾向を示しました。 全ての心血管イベント発症を合計すると、プラセボ群では32例であったのに対し、アカルボース群では15例でした。アカルボースによる治療はIGT患者において心血管イベントの相対リスクを49%有意に低下させ、絶対リスクを2.5%低下させました。 さらに心血管イベントを起こした患者の72%(プラセボ群22例、アカルボース群12例)は、糖尿病発症前のIGTの段階で心血管イベントを経験しており、残りの28%(プラセボ群10例、アカルボース3例)は糖尿病発症後に心血管イベントを発症していました。 Chiasson JL, et al. JAMA 290: 486–494,2003.")
33
MeRIA7 ~Meta-analysis of Risk Improvement under Acarbose~
2型糖尿病患者におけるα-GIの心筋梗塞発症抑制効果 (%) 対象 100 2型糖尿病患者 2,180例 アカルボース:1,248例 プラセボ:932例 α-GI 99 方法 欧米で行なわれた7つの試験(プラセボ対照無作為化二重盲検比較試験、投与期間52~164週)をメタアナリシスした. アカルボースは1回50~200mgを1日3回投与. ベイスン投与によるメリット(心筋梗塞編) 心血管イベントのうち心筋梗塞についてみると、α-GI投与はプラセボ投与に比べて長期にわたり2型糖尿病患者における心筋梗塞の発症を抑制しています。 このようにベイスンを糖尿病患者さんに併用していただくことで、糖尿病治療の目的のひとつである心血管イベントの抑制が可能になると考えられます。 是非、SU薬効果不十分例にはSU薬の増量ではなく、ベイスンを併用いただき、糖尿病治療にお役立て下さい。 非発症率 64% リスク低下 98 プラセボ 97 血糖降下作用(HbA1C) アカルボース: 8.48%→7.91% プラセボ: 8.50%→8.51% 96 p=0.0120 (日) 200 400 600 800 追跡日数 Hanefeld M. et al.:Eur. Heart J.,25,10,2004.
 対象 型糖尿病患者 2,180例. アカルボース:1,248例. プラセボ:932例. α-GI. 99. 方法. 欧米で行なわれた7つの試験(プラセボ対照無作為化二重盲検比較試験、投与期間52~164週)をメタアナリシスした. アカルボースは1回50~200mgを1日3回投与. ベイスン投与によるメリット(心筋梗塞編) 心血管イベントのうち心筋梗塞についてみると、α-GI投与はプラセボ投与に比べて長期にわたり2型糖尿病患者における心筋梗塞の発症を抑制しています。 このようにベイスンを糖尿病患者さんに併用していただくことで、糖尿病治療の目的のひとつである心血管イベントの抑制が可能になると考えられます。 是非、SU薬効果不十分例にはSU薬の増量ではなく、ベイスンを併用いただき、糖尿病治療にお役立て下さい。 非発症率. 64% リスク低下. 98. プラセボ. 97. 血糖降下作用(HbA1C) アカルボース: 8.48%→7.91% プラセボ: 8.50%→8.51% 96. p= (日) 追跡日数. Hanefeld M. et al.:Eur. Heart J.,25,10,2004.")
34
Methods 1780 eligible patients on a standard diet and taking regular exercise with impaired glucose tolerance were randomly assigned to oral voglibose 0・2 mg three times a day (n=897) or placebo (n=883) in a multicentre, doubleblind, parallel group trial. Treatment was continued until participants developed type 2 diabetes (primary endpoint) or normoglycaemia (secondary endpoint), or for a minimum of 3 years, subject to the fi ndings of an interim analysis. Analysis was by full analysis set. This trial is registered with the University Hospital Medical Information Network (UMIN) clinical trials registry, number UMIN
 or placebo (n=883) in a multicentre, doubleblind, parallel group trial. Treatment was continued until participants developed type 2 diabetes (primary endpoint) or normoglycaemia (secondary endpoint), or for a minimum of 3 years, subject to the fi ndings of an interim analysis. Analysis was by full analysis set. This trial is registered with the University Hospital Medical Information Network (UMIN) clinical trials registry, number UMIN")
35
Once the primary or secondary endpoint was achieved, patients discontinued their medication.

36
Table 1: Baseline demographic characteristics of individuals in the voglibose and placebo groups 104mg/dl 164mg/dl

37
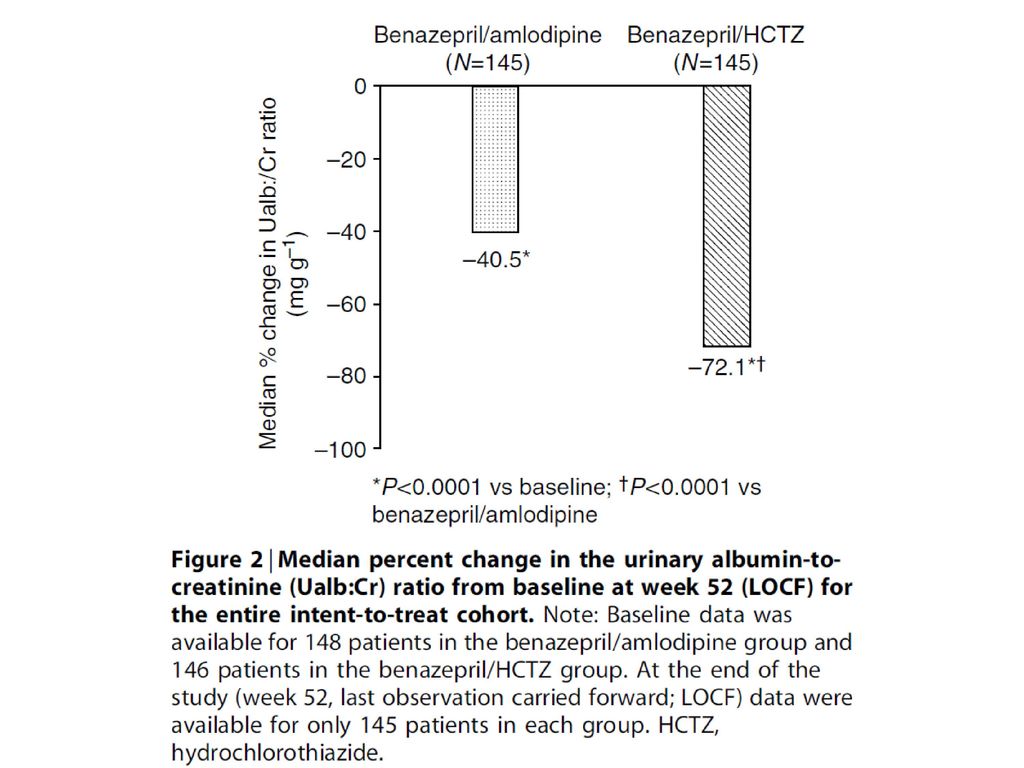
The HR was 0・577 (two-sided 95% CI 0・404–0・825; p=0・0026), verifying the efficacy of voglibose compared with placebo and, accordingly, the Independent Data Monitoring Committee made the decision to terminate the study early. The HR was 0・595 (95% CI 0・433–0・818), showing that voglibose-treated individuals had a 40・5% lower risk of developing type 2 diabetes than did placebo-treated individuals (p=0・0014) Figure 2: Effect of voglibose and placebo on the cumulative probability of individuals developing type 2 diabetes (Kaplan–Meier method)
, showing that voglibose-treated individuals had a 40・5% lower risk of developing type 2 diabetes than did placebo-treated individuals (p=0・0014) Figure 2: Effect of voglibose and placebo on the cumulative probability of individuals developing type 2 diabetes (Kaplan–Meier method)")
38
Figure 3: Effect of voglibose and placebo on the cumulative probability of individuals developing type 2 diabetes based on the number of risk factors (Kaplan–Meier method) At most two risk factors. At least three risk factors. the difference was not significant in individuals with at most two risk factors (9 vs 19 cases, 0・544, 0・258–1・147; p=0・1098). Voglibose was associated with a 39・3% risk reduction (HR 0・607, 95% CI 0・428–0・863; p=0・0053)
 At most two risk factors. At least three risk factors. the difference was not significant in individuals with at most two risk factors (9 vs 19 cases, 0・544, 0・258–1・147; p=0・1098). Voglibose was associated with a 39・3% risk reduction (HR 0・607, 95% CI 0・428–0・863; p=0・0053)")
39
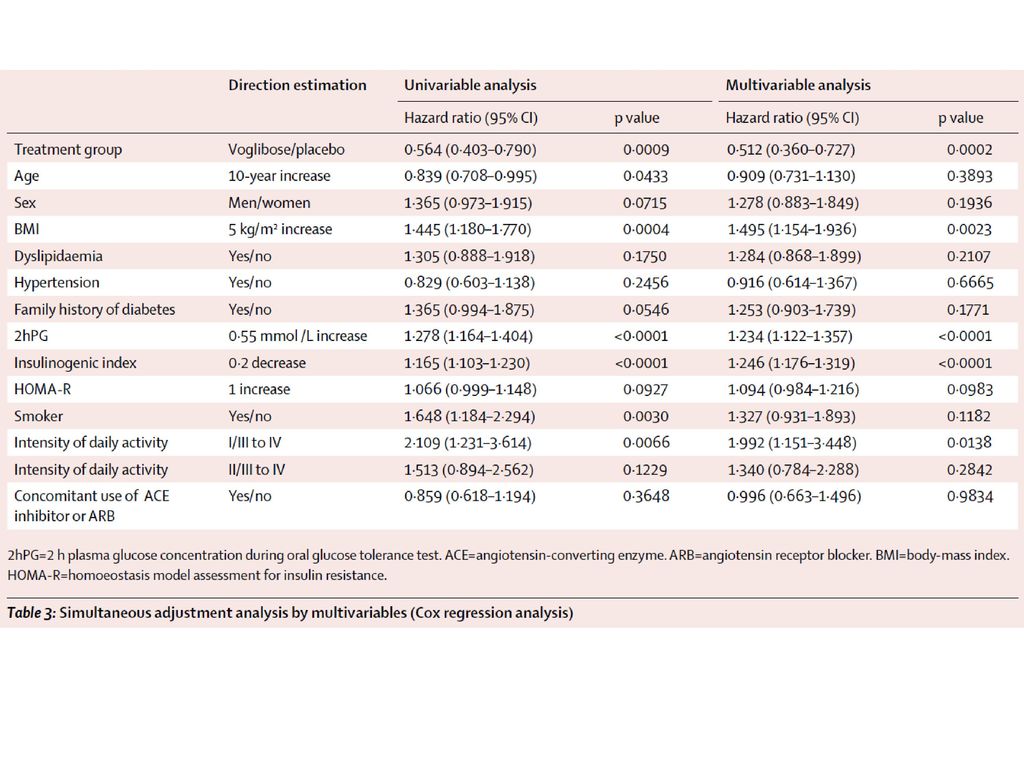
Table 2: Hazard ratio of progression to type 2 diabetes for each baseline characteristic Data are n/N, unless otherwise indicated. 2hPG=2 h plasma glucose concentration during oral glucose tolerance test. HOMA-R=homoeostasis model assessment for insulin resistance. *Percentages not calculated because reductions in number at risk depend on treatment period. †High normal blood pressure (systolic ≥130 mm Hg or diastolic ≥85 mm Hg) or being treated for hypertension. ‡Total cholesterol ≥5・7 mmol/L, triglyceride ≥1・7 mmol/L, or HDL cholesterol <1・04 mmol/L. §In a fi rst-degree or second-degree relative. 9.4mM=170mg/dl
 or being treated for hypertension. ‡Total cholesterol ≥5・7 mmol/L, triglyceride ≥1・7 mmol/L, or HDL cholesterol <1・04 mmol/L. §In a fi rst-degree or second-degree relative. 9.4mM=170mg/dl.")
41
an HR of 1・539 (95% CI 1・357–1・746; p<0・0001)
Figure 4: Effect of voglibose and placebo on the cumulative probability of individuals achieving normoglycaemia (Kaplan–Meier method) OGTT=oral glucose tolerance test.
 OGTT=oral glucose tolerance test.")
42
Table 4: Frequency of adverse events
Data are number (%). ALA=alanine aminotransferase. ASA=aspartate aminotransferase. CPK=creatine phosphokinase. GGT=γ-glutamyltransferase. *Cerebral infarction and cholecystitis in the placebo group, and cholecystitis, colonic polyp or rectal neoplasm, inguinal hernia, liver dysfunction, and subarachnoid haemorrhage in the voglibose group. †Laboratory test analyses for individuals were done at all participating centres and activities two-fold the upper limit of normal were classifi ed as increased. However, summary statistics of central laboratory data were calculated for each treatment group, and showed no variation in the laboratory data with a diff erence of one-sample t test between before and after administration (baseline at the time point of assessment).
. ALA=alanine aminotransferase. ASA=aspartate aminotransferase. CPK=creatine phosphokinase. GGT=γ-glutamyltransferase. *Cerebral infarction and cholecystitis in the placebo group, and cholecystitis, colonic polyp or rectal neoplasm, inguinal hernia, liver dysfunction, and subarachnoid haemorrhage in the voglibose group. †Laboratory test analyses for individuals were done at all participating centres and activities two-fold the upper limit of normal were classifi ed as increased. However, summary statistics of central laboratory data were calculated for each treatment group, and showed no variation in the laboratory data with a diff erence of one-sample t test between before and after administration (baseline at the time point of assessment).")
43
Findings In the interim analysis, voglibose was better than placebo (p=0・0026) in individuals treated for an average of 48・1 weeks (SD 36・3). Patients treated with voglibose had a lower risk of progression to type 2 diabetes than did those on placebo (50 of 897 vs 106 of 881; hazard ratio 0・595, 95% CI 0・433–0・818; p=0・0014). More people in the voglibose group achieved normoglycaemia than did those in the placebo group (599 of 897 vs 454 of 881; 1・539, 1・357–1・746; p<0・0001). 810 (90%) of 897 patients in the voglibose group had adverse events versus 750 (85%) of 881 in the placebo group. Serious adverse events (all one each) in the voglibose group were cholecystitis, colonic polyp, rectal neoplasm, inguinal hernia, liver dysfunction, and subarachnoid haemorrhage, and in the placebo group were cerebral infarction and cholecystitis.
 in individuals treated for an average of 48・1 weeks (SD 36・3). Patients treated with voglibose had a lower risk of progression to type 2 diabetes than did those on placebo (50 of 897 vs 106 of 881; hazard ratio 0・595, 95% CI 0・433–0・818; p=0・0014). More people in the voglibose group achieved normoglycaemia than did those in the placebo group (599 of 897 vs 454 of 881; 1・539, 1・357–1・746; p<0・0001). 810 (90%) of 897 patients in the voglibose group had adverse events versus 750 (85%) of 881 in the placebo group. Serious adverse events (all one each) in the voglibose group were cholecystitis, colonic polyp, rectal neoplasm, inguinal hernia, liver dysfunction, and subarachnoid haemorrhage, and in the placebo group were cerebral infarction and cholecystitis.")
44
Interpretation Voglibose, in addition to lifestyle modification, can reduce the development of type 2 diabetes in high-risk Japanese individuals with impaired glucose tolerance. Funding Takeda.

47
主要降圧薬の積極的適応 Ca拮抗薬 ARB/ACE阻害薬 利尿薬 β遮断薬 左室肥大 ● 心不全 ●*1 心房細動(予防) 頻脈 ●*2
狭心症 ●*3 心筋梗塞後 蛋白尿 腎不全 ●*4 脳血管障害慢性期 糖尿病/MetS*5 高齢者 ●*6 JSH2009では、第一選択薬に用いるべき薬剤として、Ca拮抗薬、ARB、ACE阻害薬、利尿薬、β遮断薬の5種類をあ げています(JSH2004からの変更点として、α遮断薬が第一選択薬から除外されています)。 種々の臨床試験の結果等を踏まえ、JSH2009では各降圧薬を用いるべき積極的適応症例をあげています。 ARBはACE阻害薬と同様に、最も幅広い患者層に対し、積極的に用いるべきと推奨されています。 特に、ARB(もしくはACE阻害薬)のみが推奨されている病態として、「心房細動(予防)」と「糖尿病/MetS」があります。 *1 少量から開始し、注意深く漸増する *2 非ジヒドロピリジン系Ca拮抗薬 *3 冠攣縮性狭心症には注意 *4 ループ利尿薬 *5 メタボリックシンドローム *6 ジヒドロピリジン系Ca拮抗薬 高血圧治療ガイドライン2009.
。 種々の臨床試験の結果等を踏まえ、JSH2009では各降圧薬を用いるべき積極的適応症例をあげています。 ARBはACE阻害薬と同様に、最も幅広い患者層に対し、積極的に用いるべきと推奨されています。 特に、ARB(もしくはACE阻害薬)のみが推奨されている病態として、「心房細動(予防)」と「糖尿病/MetS」があります。 *1 少量から開始し、注意深く漸増する *2 非ジヒドロピリジン系Ca拮抗薬 *3 冠攣縮性狭心症には注意. *4 ループ利尿薬 *5 メタボリックシンドローム *6 ジヒドロピリジン系Ca拮抗薬. 高血圧治療ガイドライン2009.")
48
POINT 6c 第6章 臓器障害を合併する高血圧 【腎疾患】
第6章 臓器障害を合併する高血圧 社内資料 POINT 6c 【腎疾患】 慢性腎臓病(CKD)患者は心血管事故のリスクが高く、早期発見がきわめて重要である。早期発見のため、全高血圧患者で検尿とeGFR(推算GFR)の算出を行う。 アルブミン尿は腎障害の進展と心血管疾患の発症に密接に関連し、アルブミン尿の減少は心腎同時保護に重要である。 降圧療法の3原則は、①降圧目標の達成、②レニン・アンジオテンシン系の抑制、③尿アルブミン、尿蛋白の減少・正常化である。 生活習慣では禁煙、食塩制限、適正体重の維持、および腎機能に応じた蛋白制限を行う。運動は腎機能に応じた指導を行う。 降圧目標は130/80mmHg未満、尿蛋白が1g/日以上なら125/75mmHg未満とする。 高血圧治療ガイドライン2009.
患者は心血管事故のリスクが高く、早期発見がきわめて重要である。早期発見のため、全高血圧患者で検尿とeGFR(推算GFR)の算出を行う。 アルブミン尿は腎障害の進展と心血管疾患の発症に密接に関連し、アルブミン尿の減少は心腎同時保護に重要である。 降圧療法の3原則は、①降圧目標の達成、②レニン・アンジオテンシン系の抑制、③尿アルブミン、尿蛋白の減少・正常化である。 生活習慣では禁煙、食塩制限、適正体重の維持、および腎機能に応じた蛋白制限を行う。運動は腎機能に応じた指導を行う。 降圧目標は130/80mmHg未満、尿蛋白が1g/日以上なら125/75mmHg未満とする。 高血圧治療ガイドライン2009.")
49
POINT 6c 第6章 臓器障害を合併する高血圧 【腎疾患】
第6章 臓器障害を合併する高血圧 社内資料 POINT 6c 【腎疾患】 ACE阻害薬、または、ARBが第一選択薬となり、尿アルブミン排泄量を指標として増量する。血清クレアチニン 2.0mg/dL以上では少量から使用し、血清クレアチニン値やK値の上昇に注意する。 多くの場合、利尿薬やCa拮抗薬との多剤併用療法が必要となる。利尿薬の使用においては、GFRが30mL/分/1.73m2以上ではサイアザイド系利尿薬、30未満ではループ利尿薬を用いる。 透析患者の降圧薬の選択時には、薬物代謝、排泄経路、透析性に注意する。 高血圧治療ガイドライン2009.

50
The primary end point was the composite of death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, hospitalization for angina, resuscitation after sudden cardiac arrest, and coronary revascularization. N Engl J Med 2008;359:

51
Background Clinical practice guidelines recommend blockers of the renin-angiotensin system alone or in combination with other agents to reduce blood pressure and albuminuria in patients with type 2 diabetes. Dihydropyridine calcium channel blockers, however, may lower blood pressure but not albuminuria in these patients. Here we tested the hypothesis that combining an ACE inhibitor with either a thiazide diuretic or a calcium channel blocker will cause similar reductions in blood pressure and albuminuria in hypertensive type 2 diabetics.

52
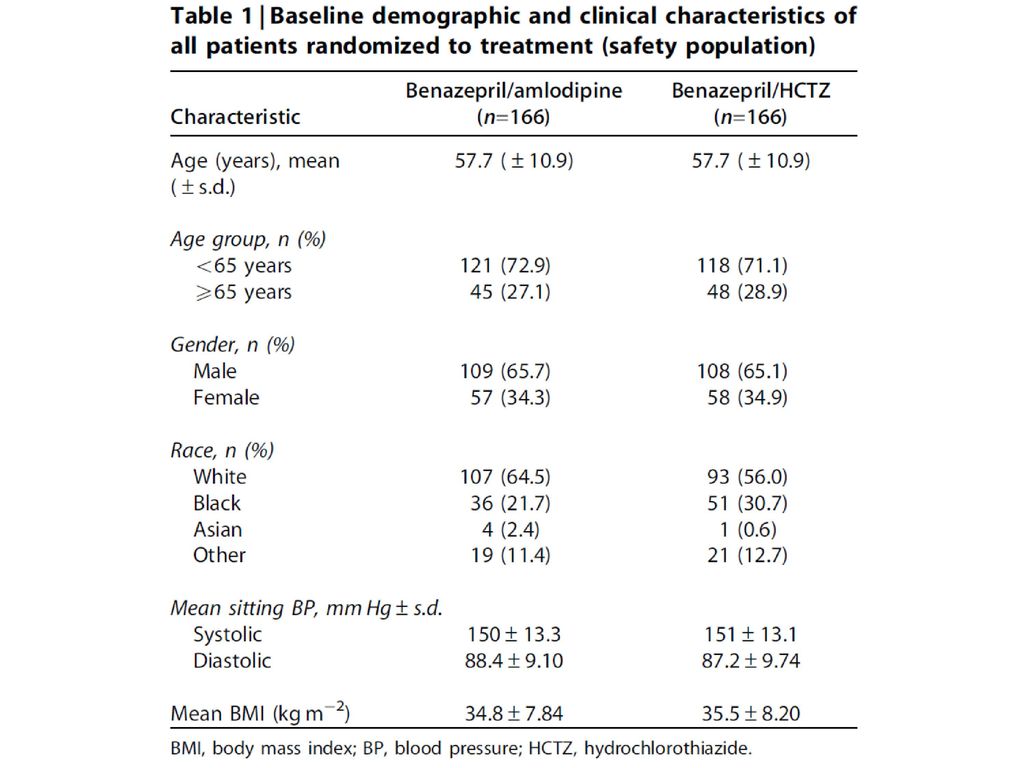
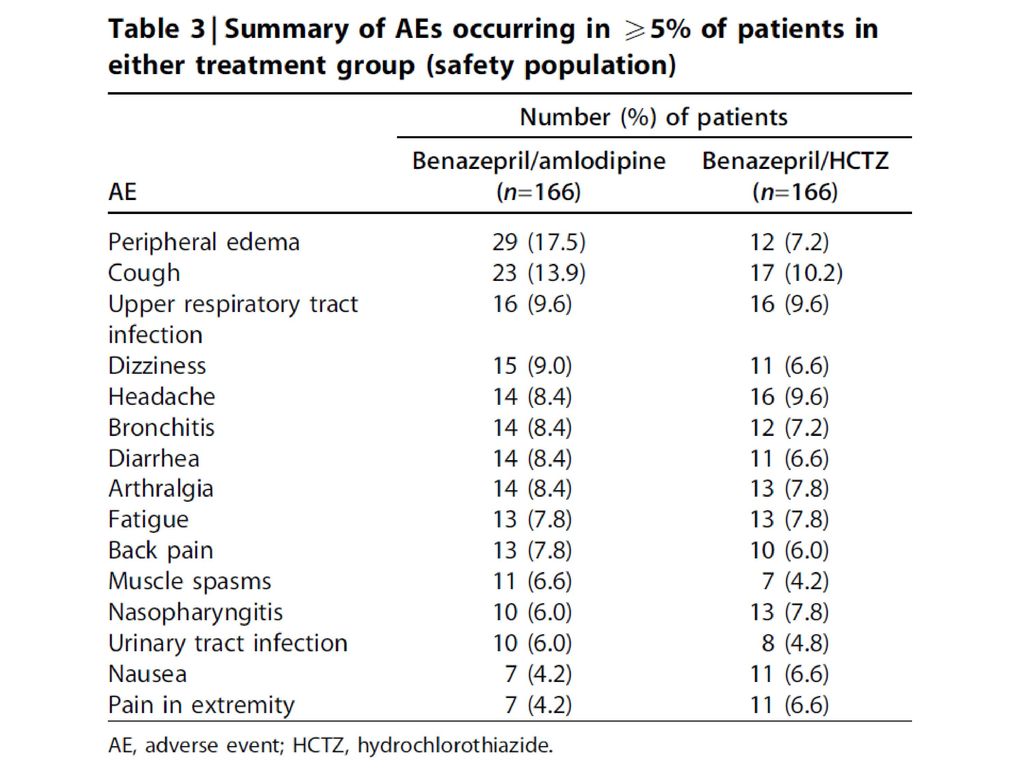
Methods We conducted a double blind randomized controlled trial on 332 hypertensive, albuminuric type 2 diabetic patients treated with benazepril with either amlodipine or hydrochlorothiazide for 1 year. The trial employed a non-inferiority design.

53
Figure 1 | Patient disposition.
aged 21–85 years with type 2 diabetes mellitus albuminuria (defined as a Ualb:Cr ratio between 20 and 500mg/gCr Hypertension: mean SBP, >130mmHg and <180mmHg mean DBP,>80mmHg and<110mmHg). At randomizeation BtA 20/5 mg or BtHCTZ 20/12.5 mg for 4 weeks to achieve the target BP of o130/80mmHg. At week 4 to BtA 40/5 mg or BtHCTZ 40/12.5 mg for additional 4 weeks. At week 8 to BtA 40/10 mg or BtHCTZ 40/25 mg in patients who had not achieved the target BP At week 12 and all subsequent visits, patients not meeting target BP were titrated to the next dose level and all patients titrated to BtA 40/10 mg or BtHCTZ 40/25 mg received add-on antihypertensives, including a-blockers, b-blockers, centrally acting antihypertensive agents, and direct vasodilators, to achieve target BP. Figure 1 | Patient disposition.
. At randomizeation BtA 20/5 mg or BtHCTZ 20/12.5 mg for 4 weeks to achieve the target BP of o130/80mmHg. At week 4 to BtA 40/5 mg or BtHCTZ 40/12.5 mg for additional 4 weeks. At week 8 to BtA 40/10 mg or BtHCTZ 40/25 mg in patients who had not achieved the target BP. At week 12 and all subsequent visits, patients not meeting target BP were titrated to the next dose level and all patients titrated to BtA 40/10 mg or BtHCTZ 40/25 mg received add-on antihypertensives, including a-blockers, b-blockers, centrally acting antihypertensive agents, and direct vasodilators, to achieve target BP. Figure 1 | Patient disposition.")
61
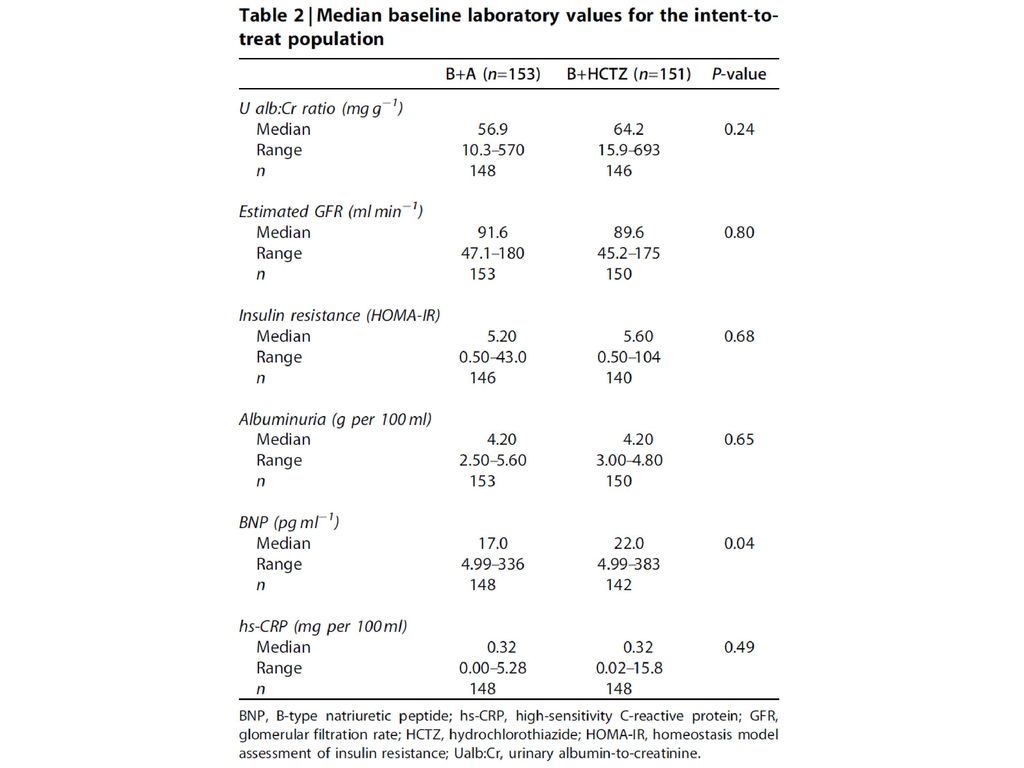
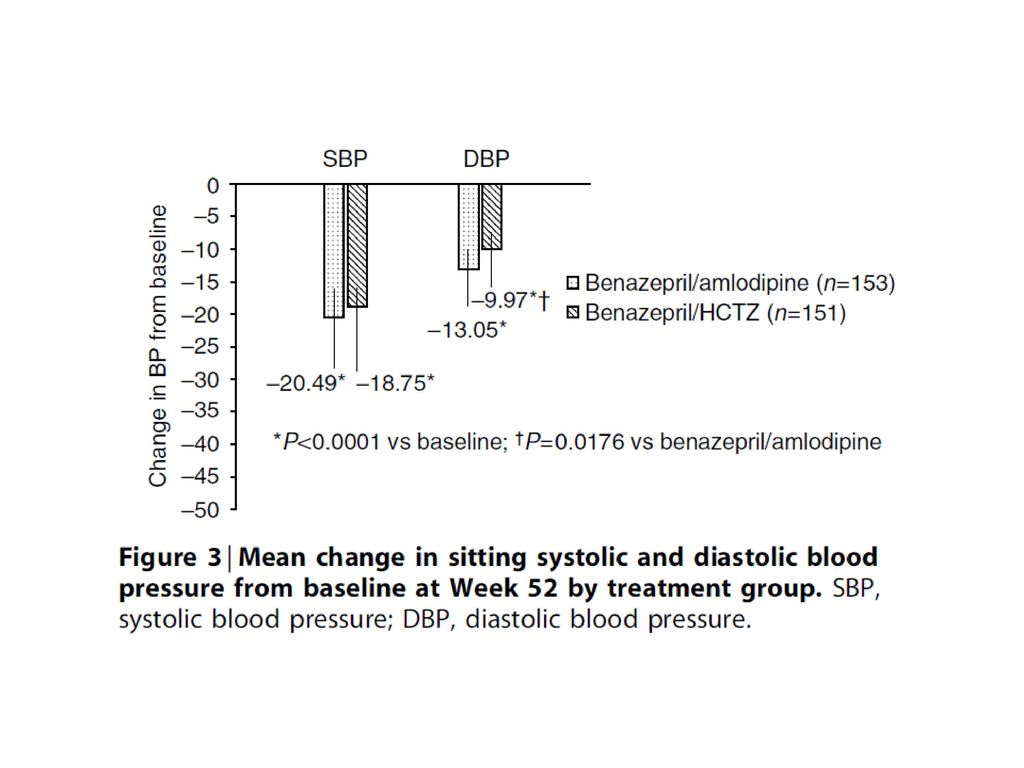
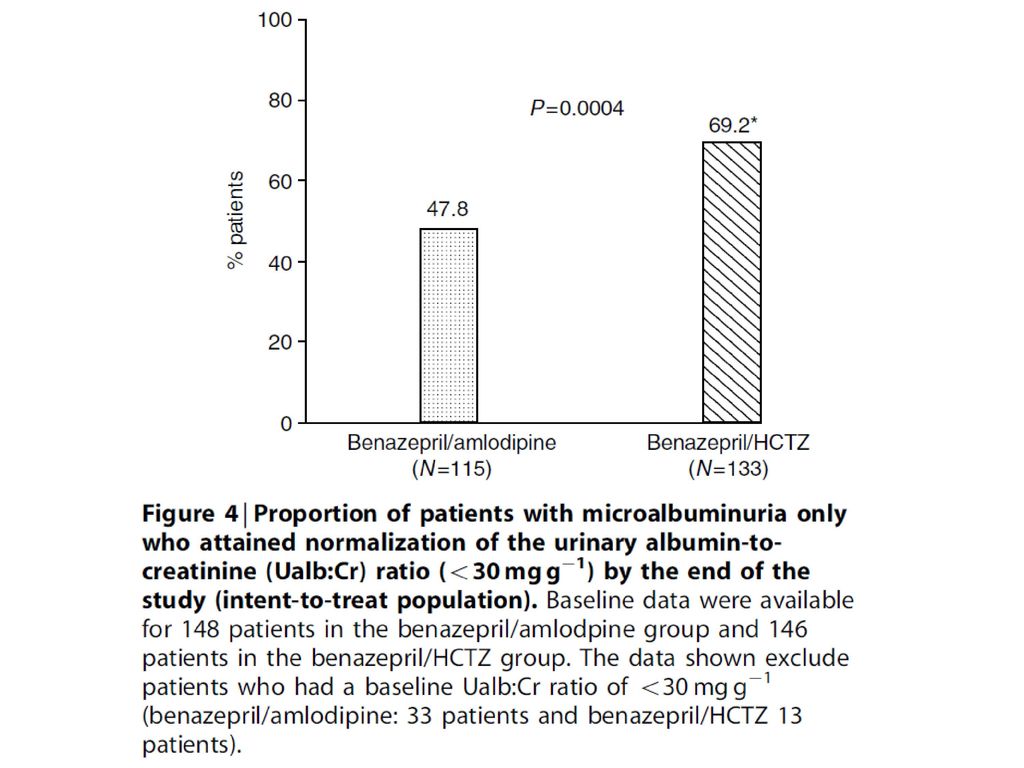
Results Both combinations significantly reduced the urinary albumin to creatinine ratio and sitting blood pressure of the entire cohort. The percentage of patients progressing to overt proteinuria was similar for both groups. When we examined patients who had only microalbuminuria and hypertension we found that a larger percentage of the diuretic and ACE inhibitor normalized their albuminuria.

62
Conclusion Interpretation
We conclude that initial treatment using benzaepril with a diuretic resulted in a greater reduction in albuminuria compared to the group of ACE inhibitor and calcium channel blocker. In contrast, blood pressure reduction, particularly the diastolic component, favored the combination with amilodipine. The dissociation between reductions in blood pressure and albuminuria may be related to factors other than blood pressure.




 脂肪組織 Plasma Glucose Blood Glucose 尿糖 血糖値は制御された値 であり制御機構が正常 なら全く血糖は上昇し.>")
, 2, 2007.>")


 (内科開業医御用達バージョン)>")
>")










 中石滋雄.>")


